
Value-Based Care Framework
A high-level overview exploring topics under the VBC umbrella
April 2020Photo: iStock.com/Natali_Mis
As we begin the Society of Actuaries (SOA) web exclusive series on the topic of value-based care (VBC), the objective of this particular article is to introduce the concept and provide the framework for two subsequent articles. Note: This information is not meant to be all-encompassing nor should one interpret the concepts and discussion to only pertain to that of a provider actuary or that of a provider. In many instances, the information can be applied broadly. It is, however, meant to provide a deeper understanding from this single perspective.
VBC DEFINED
A single definition for VBC has been elusive, since it continues to evolve and the definitions can vary depending on the stakeholder point of view. Instead of trying to create a single definition to describe VBC, it may be easier to describe it as an ideal with ambitious objectives, which is most analogous to the Triple Aim, representing improving the patient experience, reducing per-capita medical spend and improving the population’s health. These objectives are universal in nature and widely accepted by all health care stakeholders.
Applying this description to VBC provides a broad background to explore the various interrelated components necessary to achieve these objectives, which include items such as payment reform, provider and member engagement, population health management, advanced analytics, interoperability, systems integration, high-performance networks, partnership models and more. These activities, when executed at a high level and in combination with each other, will create value to the various stakeholders (such as consumers, purchasers, payers, providers) within the health care ecosystem. In this introductory article and the subsequent articles, we will take a closer look at VBC.
VBC MODELS
Moving beyond the broad and theorized definition of VBC to how it manifests in actual examples, we sometimes rationalize VBC in terms of risk-transfer models from payer to provider based on a continuum of financial risk and transformation. Exploring this approach, as shown in Figure 1, VBC can take the form of models with no downside performance risk to those with fully delegated insurance risk, and accountable services can range from process measures to bundles that are limited to services contained in a pre-defined episode of care to that of a broader total cost of care for populations.
Figure 1: Continuum of Value-Based Care Risk and Transformation
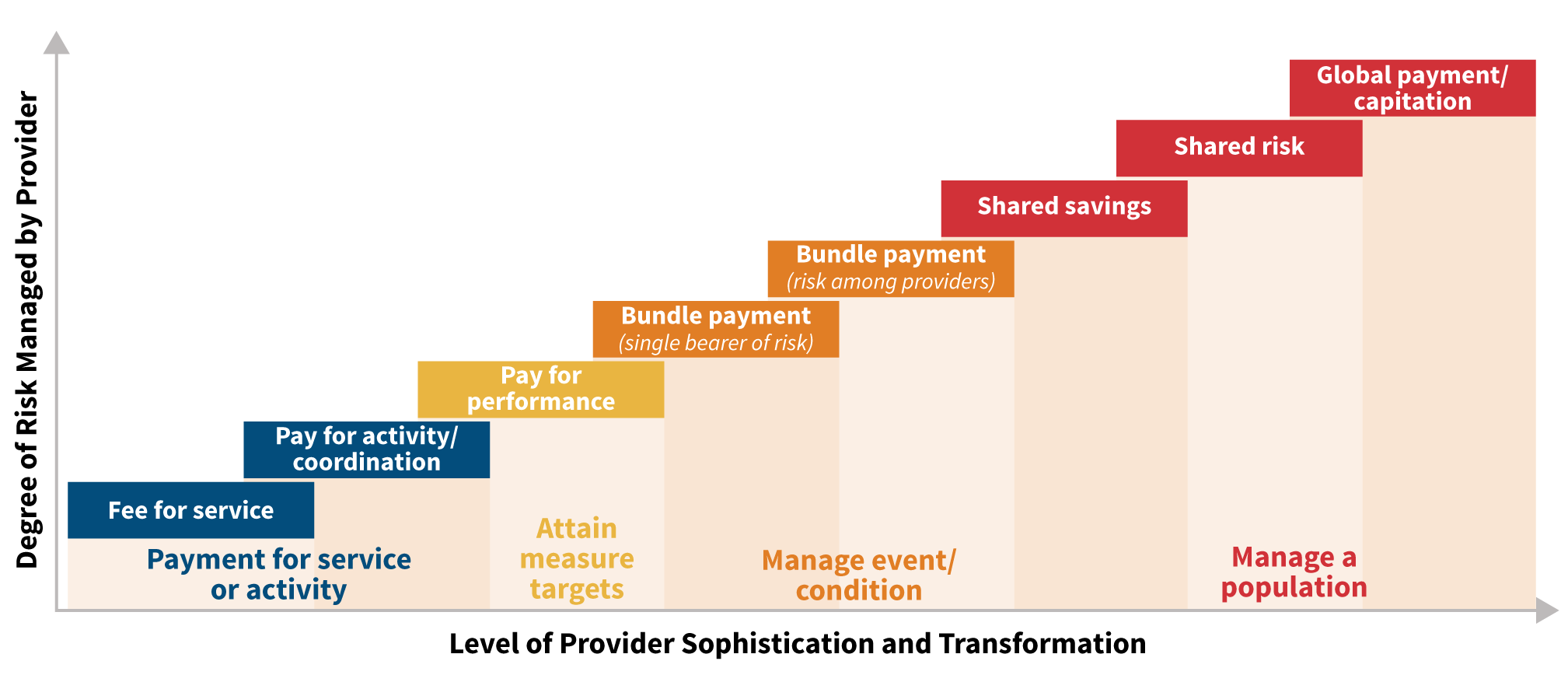
Copyright © 2017 Optum Inc. All rights reserved. Reproduced with permission.
Although the models depicted in Figure 1 suggest an almost stage-gate approach for advancing through the financial risk and transformation continuum, in reality providers contract with payer organizations using multiple arrangements listed, in many times simultaneously. Each of the models requires a multitude of capabilities that need to be flexed, dependent upon the characteristics of the models and the populations that are covered.
Figure 2 presents a VBC capabilities framework that can be used to provide guidance for any VBC model. The framework includes a range of required capabilities from strategy to operations excellence. Each of these areas should be considered with any new VBC initiative to achieve the desired outcome.
Figure 2: Value-Based Care Framework
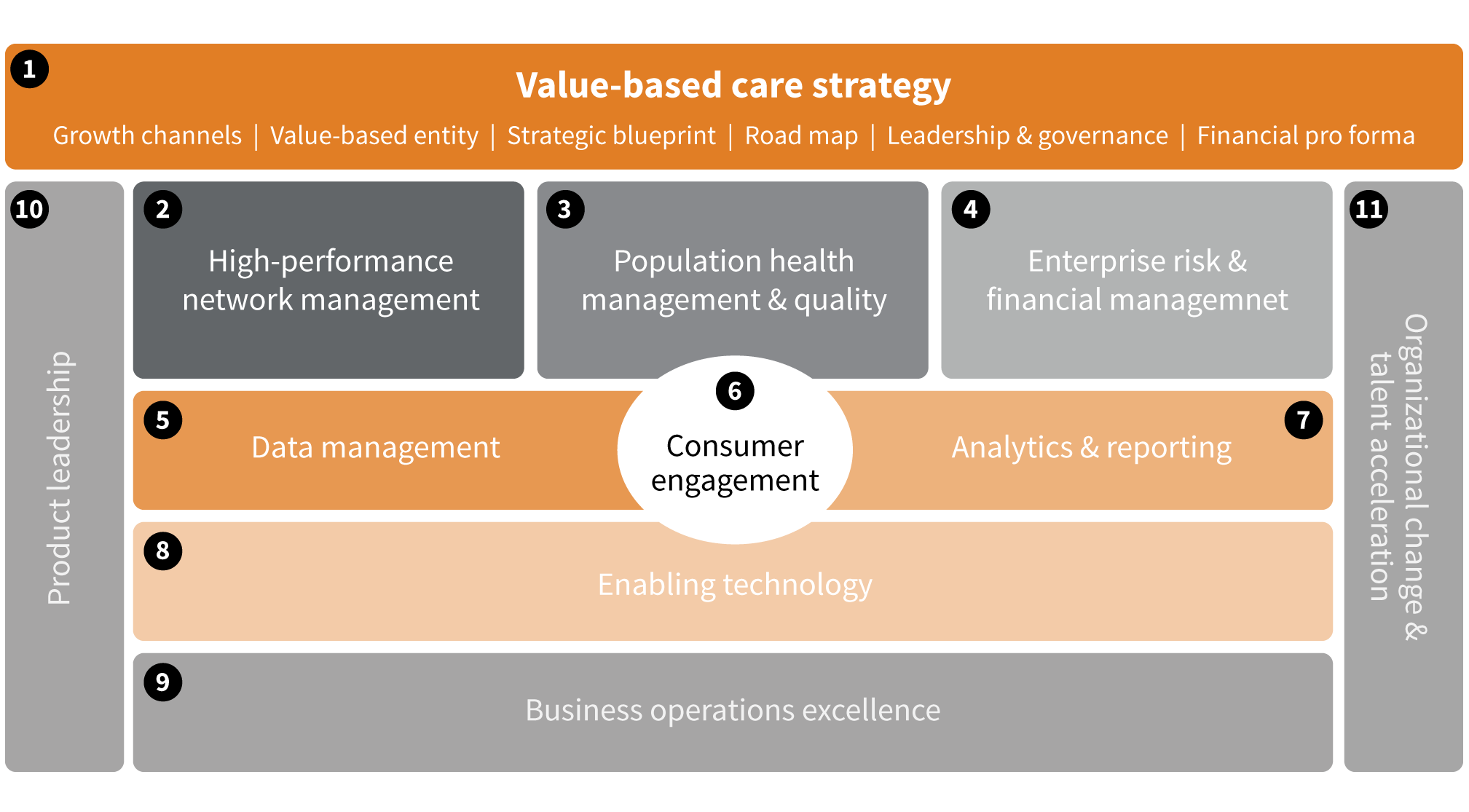
Copyright © 2017 Optum Inc. All rights reserved. Reproduced with permission.
Although fairly straightforward, there are a few areas that are worth diving further into for discussion. For any VBC model, the overall strategy should be well defined and clearly articulated in regard to growth, populations, timing, partnerships and so on. The strategy is necessary to set the vision and foundation for all other framework components.
Once the strategy has been established, then high-performing networks, population health management and enterprise financial risk management can be formulated with each of these addressed based on the unique needs of the VBC model with special consideration given to the population(s) covered. Additionally, these three areas should be addressed in combination, since any single component will be highly dependent upon the other to drive the overall success of the VBC initiative. If addressed independently, then this increases the potential for strategy and operational misalignment and thus decreases the probability of achieving the desired objectives for the VBC initiatives.
Using an example, we will explore these three critical items. Using the Centers for Medicare and Medicaid Services (CMS) Bundled Payments for Care Improvement Advanced (BPCI-A) model—which is predicated on managing the medical care and expense of an episode of care that typically involves an inpatient admission and services 90 days after discharge—a high-performing post-acute care (PAC) network is critical to the BPCI-A’s success. Obvious to the example, identifying high-performing providers in PAC delivery—such as skilled nursing facilities and home health providers, which will impact the care delivery and reduce unwarranted care variation—will have a significant impact on the program’s success.
Continuing with this example, population health management programs will need to be developed and deployed to enhance and support a patient’s care delivery within the BPCI-A program. A high focus will be on the patient’s transition from an acute care setting to PAC services, including the final move to home. Aspects such as discharge from hospital, specialist and/or primary care physician communication along with caretaker instructions and follow-up care will be critical to achieving the objectives under this model.
For the enterprise risk and financial management portion of this example, we will highlight an actuary’s ability to model, evaluate and ultimately support contracting for value under this program. Although not universal in providers’ objectives, many providers place a high priority on generating revenues and profits from entering into VBC arrangements, given that these are critical to delivering continued high-quality care to their patients. Under the BPCI-A example, the review and modeling of the program to identify and contract with CMS for the individual bundles that have the highest probability of financial success is an essential first step. Then, offsetting the potential revenues with the cost and deployment of population health management programs along with the cost to engage the PAC or other providers need to be considered to ultimately inform a provider’s decision to participate in this program.
Additional margins from decreasing the internal costs to deliver the services may also be considered within the context of the program (such as lower costs for devices with similar or better outcomes). We explore more aspects of enterprise risk and financial management in another article in this series (and in an upcoming issue of Health Watch) and how actuaries support developing and optimizing this important aspect of a VBC initiative.
In addition to these areas within the framework, there are others key aspects that need to be considered for any VBC initiative. In Figure 3, we have provided summary-level information about these to help define each area and its key components.
Figure 3: Value-Based Care Framework Capabilities Summary
| Overview | Key Components | ||
| 1 | Value-based care strategy | Defines objectives and quantifies impact to organization; addresses the why, what, when, who and where | Target populations and geographies; quantifies key performance measures; pro-forma(s) development; capability assessments and road map development |
| 2 | High-performance network management | The composition and delivery of high-quality, efficient care by the provider network necessary to support the VBC strategy | Provider composition and network inclusion; key performance measurements (site of care, total cost of care, episodic, service category utilization); internal cost and outcome variation analyses; referral management; provider/utilization demand forecasting; engagement and compensation models |
| 3 | Population health management and quality | The development and deployment of care management programs necessary to support the high-performing network in addressing the overall needs of the target populations | Care management program stratification, identification and development (e.g., transitions of care, chronic care management, pain management, oncology home); member and provider engagement models and key performance measurements; care pathways development and deployment |
| 4 | Enterprise risk and financial management | The enterprise financial risk management of the VBC contracts both upstream with payers and downstream with providers | Feasibility analyses and contract forecasting revenue and margin models; payer/provider and provider/provider contracting support (e.g., VBC and fee-for-service contracts); internal cost modeling; market share growth and share of wallet strategy support; risk mitigation; and reinsurance/excess of loss (spec and aggregate) models |
| 5 | Data management | Data governance and management to support VBC performance management process | Strategy, security, acquisition, deployment and governance for claims; clinical (e.g., electronic health records (EHR)), operational and supplemental data (e.g., social determinants of health) |
| 6 | Consumer engagement | Various consumer engagement methods to support better care delivery and improvement in overall health outcomes | Stratification and identification of key behavioral engagement activities to engage various consumer cohorts (e.g., chronically ill, healthy member, acute conditions) |
| 7 | Analytics and reporting | Analytics required to support the development and execution of the VBC strategy and performance management process | Strategy; provider network; population health; financial risk; predictive and margin analytics; and reporting to support decision support; and resource allocation to improve the VBC performance of the organization |
| 8 | Enabling technology | Technology that enables better care delivery and improvement in overall health outcomes | Patient capture information (i.e., EHRs); population health analytic platforms; systems integration; cost accounting solutions; embedded software solutions; artificial intelligence and machine learning applications |
| 9 | Business operations excellence | Development and implementation of continuous improvements in VBC operations | Identification, development and execution of operational improvements to drive value through the VBC activities |
| 10 | Product leadership | Dedicated leadership with responsibility and accountability for the development of new initiatives to support the organization’s VBC and product strategy | Develop, communicate and execute vision and road map for VBC growth and targeted success factors; lead and influence others within or outside organization to achieve results |
| 11 | Organizational change and talent acceleration | Acquisition and deployment of people and processes to execute the development of a new product to support the organization’s VBC and product strategy | Identify required skill sets to support VBC and product strategy; assess current talent and determine gaps; develop gap closure plans; recruit new and retain top talent |
As shared previously, the objective of this article is to provide the introductory foundational aspects for further exploration within the context of a VBC framework. Although actuaries can and do play critical roles and provide significant contributions in each of the capabilities within the VBC framework, subsequent articles in this series examine key considerations primarily focusing on the enterprise risk and financial management aspects of VBC programs.
Copyright © 2020 by the Society of Actuaries, Chicago, Illinois.